Long Term Care Policy Cap That Triggers After a Single Nursing Home Bill
Long-term care insurance is sold as a safety net for the years when you cannot dress, bathe, or feed yourself. Insurers promise: pay premiums now, get coverage later. The advertised lifetime cap—often $300,000, $400,000, or more—sounds like a generous cushion. But that number can vanish faster than most buyers realize. A single nursing home stay, at today's rates, can push against that ceiling in under three years. By the time policyholders discover the gap, they are already in the middle of a crisis.
This is not an argument against planning for long-term care. It is an argument for understanding the specific financial instrument you are buying. The fine print—daily benefit limits, elimination periods, narrow definitions of covered care—determines whether the policy pays out when it matters. If you are evaluating a policy today, the first question should not be "What is the lifetime maximum?" It should be "How fast can that maximum be consumed by the actual cost of care in my area?"
The Policy Promise That Breaks on First Use
The headline number on a long-term care policy is typically the lifetime maximum benefit. A policy might say "$365,000 lifetime maximum" in bold letters on the first page. That figure is meant to reassure you that even a catastrophic stay is covered. But the daily cost of a semi-private room in a nursing home now runs between $400 and $800 in most regions, with some metropolitan areas exceeding $1,000 a day. At $600 per day, a $365,000 cap is exhausted in roughly 608 days—less than two years. The median length of stay in a nursing home is about 2.5 years, according to industry data. For those with chronic conditions, stays of three to five years are common.
The math is brutal: if you buy a policy at age 60 and need care at age 80, the cap that seemed adequate at purchase may cover only a fraction of the actual stay. Inflation in healthcare costs runs well above general inflation. A policy bought in 2010 with a $300,000 cap would have covered roughly three years of care at that time. By 2025, the same $300,000 buys about 18 months in many markets. The cap is not adjusted for the timing of the claim. It is a fixed dollar amount that erodes in real value every year you delay a claim.
Sales illustrations often show the cap as a pool of money that grows if you do not use it. Some policies do include an automatic inflation rider, but it is often optional and comes at a significant premium. Many buyers skip it to keep monthly costs low. Without it, the cap stays flat while the cost of care rises. The result is a policy that looks adequate on paper at purchase but becomes progressively insufficient with each passing year. Policyholders discover this only when they submit a claim and the daily benefit runs out months earlier than expected.
Industry data from the American Association for Long-Term Care Insurance suggests that roughly one in four claims exceeds the policy's lifetime maximum. That means a quarter of policyholders who actually use their insurance hit the cap before care ends. They are then left paying out-of-pocket for the remainder of their stay, often at the worst possible time—when savings are already depleted from the earlier portion of care. The cap that was supposed to protect them becomes a ceiling that forces them into financial freefall.
How Insurers Structure the Cap to Minimize Payouts
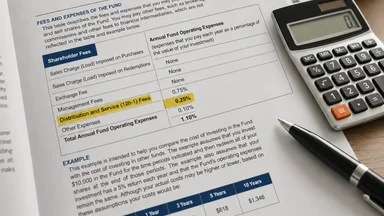
The lifetime maximum is not the only limit. Insurers layer multiple constraints that together determine how much they actually pay. The daily benefit—say $200 or $300 per day—is the amount the policy pays for each day of covered care. The lifetime maximum is calculated as the daily benefit multiplied by the number of days of coverage. A policy with a $200 daily benefit and a 1,825-day benefit period (five years) has a $365,000 lifetime maximum. But if the actual cost of care is $600 per day, the policy pays only $200 per day, and the policyholder must cover the $400 difference out-of-pocket. The cap is consumed at the daily benefit rate, not at the actual cost rate. So the policyholder burns through the cap more slowly than the full cost of care, but the uncovered gap is enormous.
The elimination period is another structural feature that delays the start of benefits. Most policies require you to pay for the first 30, 60, or 90 days of care out-of-pocket before the policy begins paying. This is essentially a deductible. Some policies count only calendar days of care toward the elimination period, while others count only days on which you actually receive services. If you are in a facility but not receiving skilled care on a given day, that day may not count. The elimination period can stretch far beyond the stated number of days, especially for home care where visits are intermittent. By the time the policy starts paying, you may have already spent tens of thousands of dollars.
Inflation riders, when available, are often capped. A typical compound inflation rider increases the daily benefit by 3% or 5% per year, but the lifetime maximum also increases at that rate. However, many policies cap the total increase at 100% or 200% of the original benefit. After that, the benefit stops growing even if costs continue rising. Other policies offer a simple inflation rider that increases the benefit by a fixed percentage each year, but the increase is not compounded. Over 20 years, the difference between simple and compound inflation is substantial. A $200 daily benefit with 5% simple inflation after 20 years becomes $400 per day. With 5% compound inflation, it becomes roughly $530 per day. Most buyers do not realize which type they have until they file a claim.
Shared-care provisions, which allow a couple to pool their benefits, are available but rare in standard contracts. They require an additional rider and higher premiums. Without shared care, if one spouse exhausts their cap and the other never needs care, the unused benefits are lost. This asymmetry is a feature, not a bug. It allows insurers to keep premiums lower by assuming that not all policyholders will use their full benefit. The actuarial tables are built on average stays, not maximum possible stays. The cap is designed to cover the average, not the outlier. But when you buy insurance, you are insuring against the outlier—the long stay that would otherwise wipe out your savings. The cap structure works against that purpose.
The Fine Print Most Buyers Never Read
Definitions matter in insurance contracts, and long-term care policies are dense with them. The term "skilled care" is often narrower than what a typical nursing home resident receives. Many policies cover only care that requires a licensed nurse or therapist and is ordered by a doctor. Custodial care—help with bathing, dressing, eating, and toileting—may be excluded or covered only at a reduced daily rate. Yet the majority of nursing home residents need custodial care, not skilled care. If your policy defines covered care narrowly, you may find that much of your stay is not reimbursed, even if you are inside the facility.
Home care is typically counted at a lower daily rate than facility care. A policy might pay $200 per day for nursing home care but only $100 per day for home health aide visits. The lifetime maximum is the same, but home care consumes it more slowly—provided the aide visits are frequent enough. However, many policies limit the number of home care visits per week or the total number of hours per day. If you need round-the-clock care at home, the daily benefit may cover only a fraction of the cost. The policy's structure assumes that home care is cheaper and less intensive, which is not always true for someone with advanced dementia or multiple chronic conditions.
Benefit period reset clauses vary by carrier. Some policies allow the benefit period to reset after a certain number of days without care—say, 180 days. If you use care for six months, then go without care for six months, the benefit period restarts. Others do not reset at all; once you use a day of benefit, it is gone forever. The reset feature is valuable, but it is not standard. You have to ask for it and read the contract to confirm. Agents may mention it in passing but rarely highlight the conditions under which it applies. If you have a progressive condition like Parkinson's or Alzheimer's, you are unlikely to have a 180-day gap in care, so the reset is effectively useless.
Pre-existing condition exclusions can linger for six months or longer after the policy is issued. If you are diagnosed with a condition during that period, any care related to that condition may be excluded permanently. Some policies waive the exclusion if the condition was disclosed on the application, but others do not. The application process itself is a trap: if you fail to disclose a minor ailment that later becomes relevant, the insurer can deny coverage for misrepresentation. The fine print is not just about what is covered; it is about what can void coverage entirely. Renewal guarantees are another area of confusion. Most policies are "guaranteed renewable," meaning the insurer cannot cancel your coverage as long as you pay premiums. But they can raise premiums with state approval. Rate increases of 50% or more have been common in recent years, forcing some policyholders to drop coverage they can no longer afford.
Comparing LTC Insurance to Other Financial Instruments
Given the limitations of a capped long-term care policy, it is worth considering alternatives. Home equity is one of the largest assets many retirees hold. A reverse mortgage or home equity line of credit can provide funds to pay for care without draining investment accounts. The proceeds are generally tax-free because they are loan advances, but the loan must be repaid when the home is sold. For someone who plans to stay in the home, this can be a viable way to fund in-home care. The catch is that the home must be in good condition and the borrower must keep up with property taxes and insurance. If the home declines in value or the borrower cannot maintain it, the strategy fails.
Life insurance policies with cash value can be tapped for long-term care needs. Some policies include a long-term care rider that accelerates the death benefit if you become chronically ill. The advantage is that you are using money you already have, not paying premiums for a separate policy. The disadvantage is that the cash value may be far less than the cost of extended care. A $100,000 life insurance policy with a long-term care rider might provide $200,000 in benefits, but that is still a fraction of what a multi-year stay costs. You are essentially converting a death benefit into a living benefit, which reduces what your heirs receive.
Annuities can also be structured to provide a steady income stream that covers care costs. For instance, a single-premium immediate annuity (SPIA) can guarantee a monthly payment for life. If you need care, that income can go directly to the facility. The risk is that you are locking up a lump sum that could otherwise be used for other needs. Inflation is also a concern: a fixed annuity payment loses purchasing power over time. Some insurers offer inflation-adjusted annuities, but the initial payout is lower. A 2023 study by the Society of Actuaries found that a 65-year-old purchasing a $200,000 SPIA with a 3% annual increase would receive about $1,100 per month initially, which would cover only part of a nursing home's daily rate. The trade-off is between certainty and flexibility.
Self-insuring—relying on your own savings and investments—is a strategy that works for those with substantial assets. A diversified portfolio of stocks and bonds can be drawn down to pay for care. The advantage is that you keep control of the money and avoid insurance premiums that may never pay out. The risk is that a long stay could deplete your portfolio earlier than planned, leaving you with little for other retirement expenses. To self-insure safely, you need enough assets to cover a worst-case scenario—say, five years of care at $100,000 per year, or $500,000 in today's dollars, plus a buffer for inflation. That is beyond the reach of most households. Medicaid spend-down remains the last resort for those who exhaust their assets. It requires you to spend down to roughly $2,000 in countable assets (in most states) before the government pays for care. The process is complex and varies by state, and not all facilities accept Medicaid. It is a safety net, but one with significant holes.
Real-World Case: The $400,000 Bill That Broke the Cap
Consider the case of a 72-year-old woman in the Midwest who entered a skilled nursing facility in 2023 after a stroke left her unable to walk or feed herself. She had purchased a long-term care policy in 2005 with a $365,000 lifetime maximum and a $200 daily benefit, with no inflation rider. The policy had a 90-day elimination period. During those first three months, she paid roughly $27,000 out-of-pocket based on the facility's daily rate of $300. After the elimination period, the policy began paying $200 per day, leaving her with a $100 daily gap. The facility's rates increased annually by about 5%, so by year two, the daily rate was $315, and her daily gap had grown to $115.
By the end of the third year, her total out-of-pocket costs—including the elimination period, the daily gaps, and uncovered services like physical therapy—exceeded $100,000. Her policy's lifetime maximum was exhausted after exactly 1,825 days of benefit payments (five years of $200 per day), but she had only been in the facility for three years because the daily benefit was less than the actual cost. In reality, the cap was consumed faster than the calendar: each day of care used one day of benefit, but the benefit amount was fixed while costs rose. She hit the cap after 1,825 days of benefit payments, which corresponded to about three years of actual care because the policy paid only a portion of each day's cost. The math is confusing, but the result is clear: she was left with a care bill of over $100,000 after the policy stopped paying, and she still needed care. Her family had to sell her house to cover the gap.
This case is not unusual. A 2024 study by the Employee Benefit Research Institute found that roughly 20% of nursing home stays exceed three years. For those with chronic conditions like dementia, the percentage is higher. The policy she bought in 2005 seemed adequate at the time. The lifetime cap of $365,000 was roughly three times the annual cost of care in her area then. By 2023, annual costs had nearly tripled, but her cap had not budged. The policy was designed for a world that no longer exists. The insurer had approved the policy based on actuarial assumptions that did not account for the rapid inflation in healthcare costs over the following two decades.
The lesson is not that long-term care insurance is worthless. It is that the specific terms of the contract—the daily benefit, the inflation rider, the elimination period—determine whether the policy will actually cover a catastrophic stay. A policy with a $500 daily benefit and a compound inflation rider would have covered her care for much longer. But that policy would have cost two to three times as much in premiums. The trade-off is real. The woman in this case chose a cheaper policy to keep premiums affordable, and it failed her when she needed it most. The industry calls this "buyer beware." But buyers are rarely given the tools to evaluate the risk.
What to Look for Before Buying a Policy
If you are considering a long-term care policy, start by comparing the lifetime cap to the daily benefit structure. A high lifetime cap is meaningless if the daily benefit is too low to cover a significant portion of the actual cost. Look at the daily benefit in relation to the average cost of a semi-private room in your area. The National Investment Center for Seniors Housing & Care (NIC) publishes annual cost data in its Market Fundamentals reports. If the daily benefit covers less than 50% of the local average, you are essentially buying a discount card, not insurance. The policy will delay the financial hit but not prevent it.
Check the compound inflation protection terms carefully. Ask whether the rider is automatic or optional, what percentage it increases by, and whether there is a cap on total growth. A 3% compound rider doubles the benefit in about 24 years. A 5% compound rider doubles it in about 14 years. If you are buying at age 60 and expect to claim at age 80, the 5% rider is far more valuable. But it also costs more. Some policies offer a "future purchase option" that allows you to buy additional coverage at specified intervals without medical underwriting. This can be a cheaper way to get inflation protection, but you must remember to exercise the option.
Verify nonforfeiture benefits. If you stop paying premiums because you can no longer afford them, a nonforfeiture rider ensures you get some reduced benefit based on the premiums you have already paid. Without it, you lose everything. The rider adds to the premium, but it is worth considering if there is any risk of lapse. Also ask about waiver of premium: once you are receiving benefits, most policies waive the premium. That is standard, but confirm it in writing.
Request benefit trigger examples from the insurer. Ask them to walk you through a scenario where a policyholder with a specific condition—say, a hip fracture or early-stage Alzheimer's—qualifies for benefits. The trigger is usually based on needing assistance with at least two of six activities of daily living (bathing, dressing, eating, toileting, transferring, and continence) or having a severe cognitive impairment. But the documentation required can be onerous. Some insurers require a nurse assessment every 60 days to continue benefits. If you miss a deadline, benefits can stop. Understanding the administrative burden is as important as understanding the dollar amounts.
Run your own cost projection using local rates. Do not rely on the agent's illustration. Take the daily benefit, multiply it by 365, and compare that to the annual cost of a nursing home in your area. Then apply the inflation rider to both sides for the number of years until you expect to claim. If the policy's annual benefit covers less than 80% of the projected cost, you are likely to face a significant gap. The exercise is sobering, but it is better to know now than to discover it when you or a parent is in the facility.
The Regulatory Gap That Lets This Persist
State insurance departments are responsible for regulating long-term care policies, but they lack uniform standards for cap adequacy. The National Association of Insurance Commissioners (NAIC) has a model act that recommends certain disclosures, but it is not mandatory in most states. As a result, policies vary wildly in how they present the cap and whether they require inflation protection. Some states require insurers to offer an inflation rider, but they do not require the buyer to accept it. Most buyers decline it to save money. The agent has an incentive to keep the premium low to close the sale. The result is a market where a large portion of policies sold are structurally inadequate for the risk they are supposed to cover.
Rate increase approvals are another weak point. Insurers must get state approval to raise premiums on existing policies, but the approval process rarely considers whether the original cap was adequate. The focus is on whether the increase is justified by claims experience, not on whether the policy will still provide meaningful coverage after the increase. Policyholders who face a 50% premium hike often let the policy lapse, which is exactly what the insurer wants. The cap never triggers because the policy is gone. The regulatory system does not account for this dynamic. It treats each rate filing in isolation rather than looking at the long-term viability of the coverage.
Consumer disclosures are supposed to help buyers understand what they are purchasing, but they are often generic. The NAIC's Shopper's Guide to Long-Term Care Insurance includes a worksheet for comparing policies, but it does not require a scenario analysis that shows how quickly the cap would be exhausted at current local costs. Some states have adopted more stringent requirements, such as California's requirement that insurers provide a "benefit illustration" showing the projected daily benefit and lifetime maximum at age 85 assuming 5% inflation. But even that illustration is based on assumptions that may not hold. A MarketWatch article from June 2023 titled "The Hidden Cost of Long-Term Care Insurance" noted that many consumers are unaware of assistance programs like Medicaid or state-specific waiver programs that could help cover costs not paid by insurance. The combination of poor policy design and weak regulation leaves consumers exposed.
There is no easy fix. Mandating inflation protection would raise premiums and price out lower-income buyers. Requiring higher daily benefits would do the same. The tension between affordability and adequacy is inherent. But the current system tilts too far toward affordability at the point of sale, leaving policyholders with a false sense of security. A reasonable step would be to require insurers to show, at the time of purchase, a simple chart comparing the policy's projected coverage at age 80 or 85 to the projected cost of care in the buyer's area, assuming 3% and 5% inflation. That would at least put the gap in plain view. Until that happens, buyers must do the math themselves.
The Counter-Argument: When Insurance Still Makes Sense
Despite the structural flaws, long-term care insurance can still be a rational choice for a specific subset of buyers. For households with assets between roughly $150,000 and $1.5 million—too much to qualify for Medicaid but not enough to self-insure comfortably—a policy can prevent a catastrophic stay from wiping out a lifetime of savings. The key is to buy a policy that matches the risk. A policy with a high daily benefit (say, 80% of local nursing home costs) and a compound inflation rider, even with a shorter benefit period of three years, may be more useful than a policy with a low daily benefit and a high lifetime cap. The goal is not to cover every possible day of care, but to buy enough time to arrange other resources—selling a home, tapping family support, or transitioning to a lower-cost setting—without financial panic.
For those who cannot afford a robust policy, the alternative is not necessarily self-insurance. It is a deliberate plan that includes home equity, family contributions, and a clear understanding of Medicaid rules. Insurance can be part of that plan, but only if the buyer understands that the cap is a ceiling, not a safety net. The industry markets the cap as a limit of liability, but buyers treat it as a promise of full coverage. The disconnect is dangerous. A policy that covers three years of care at 80% of cost is a useful bridge. A policy that covers 18 months at 50% of cost is a placebo. The difference is in the details.
In the end, the decision to buy long-term care insurance is a bet on the probability of a long stay. The cap structure means that the bet is often against the buyer. But for those who cannot absorb a $200,000 or $300,000 care bill, even a partial payout can make a difference. The trick is to buy enough coverage to matter, and to do the math before the crisis hits. Know the difference between a fortress and a picket fence before you sign.
This article is for informational purposes only and does not constitute financial, legal, or insurance advice. Consult a qualified professional for guidance specific to your situation.